Asthma is a common breathing condition. It affects the small and medium-sized airways (bronchi) in the lungs.
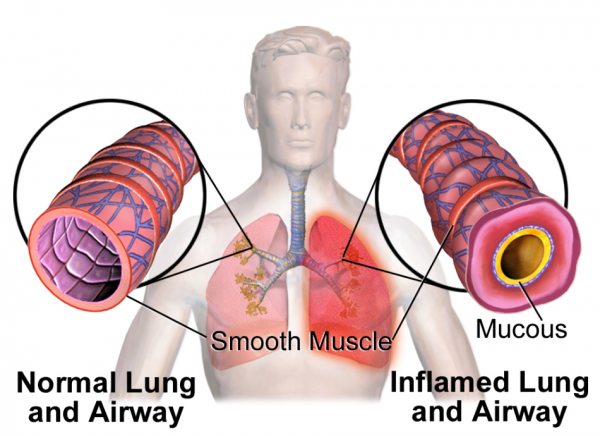
In asthma, your child's airways are inflamed and there is:
swelling of the airway wall
an increase in mucus or phlegm
tightening of the muscle in the airway wall.
These changes cause narrowing of your child's airways. This leads to wheezing, cough and difficulty with breathing.
Wheezing is a musical, whistly sound that tamariki make, usually when breathing out. It can also happen when they breathe in. The sound comes from their chest, not from their nose or throat.
The image below shows a normal airway and the airway of a person with asthma.
One in 4 tamariki in Aotearoa New Zealand will have asthma at some time during childhood. It's not clear why some children have asthma when others don't.
there is asthma in the family – parent, brother or sister
one or both parents have an allergic condition, eg, asthma, hay fever or eczema.
Modern Western lifestyle may play a part in the rise in asthma that has happened over the last few decades. Changes in housing, diet and a more hygienic environment may contribute. Outdoor environmental pollution may make asthma symptoms worse but it doesn't actually cause asthma. Experts continue to study the reasons for the increase in asthma.
Tamariki and rangatahi with asthma have airways that are sensitive and react to certain triggers. Some children have asthma all year round. Others may only have it in certain seasons or situations.
Things that can cause an attack include the following:
Infections: Viruses like colds and the flu can cause some children to have worse asthma symptoms which may lead to an asthma attack.
Allergies: If your child is allergic to things like pollens, grass, dust or pet fur, this can worsen their asthma.
Irritants: Irritants may trigger asthma attacks. Examples or irritants are air pollution, car exhaust, vapours and mouldy environments.
Tobacco smoke: Tobacco smoke can trigger asthma attacks and can make your child's asthma symptoms worse. All tamariki need a smoke-free environment, wherever they happen to be.
Exercise: Exercise and physical activity are a big part of helping tamariki stay healthy and fit. Exercise is also an important part of asthma management. But, sometimes exercise or activity can trigger an episode of asthma.
Changes in the weather: Some children may find a change in the weather or certain conditions, like cold or damp weather, can make their asthma worse.
Other things that can help your child's asthma include:
living in a smoke-free environment at all times
keeping your house warm and dry
where possible, avoiding things that trigger their asthma.
Be smoke-free
Make sure your child's environment is smoke-free, wherever they happen to be. Asthma increases in tamariki whose parents smoke. Tobacco smoke also triggers asthma attacks and makes a child's asthma more severe. Many environmental factors contribute to asthma. Cigarette smoke is one that you can avoid.
If you want to give up smoking:
call the free Quitline on 0800 778 778 or text 4006
Keep a symptom diary and a record of possible triggers
Asthma symptoms and triggers may differ from child to child and from time to time. It is useful to know your child's triggers. Use a symptom diary to keep a record of possible triggers.
You should see your healthcare provider and ask about asthma if your child:
wheezes and coughs with a cold (virus)
wheezes and coughs after exercise
wheezes and coughs during the night
can't keep up when they're running around with children of the same age
says they are out of breath or breathless
complains they feel tired or asks you to carry them (depending on their age) when you go for a walk
doesn't run around as much as other children of the same age.
These are some of the symptoms of asthma in children, but they may also be due to other less common conditions. Talk to your healthcare provider about them.
Asthma is a long-term condition. The majority of children with asthma have less troublesome asthma as teenagers. Symptoms can appear again in adulthood. If your child has severe asthma, it's more likely to continue or return in later life.
Your child should learn about asthma and gradually take over responsibility for its management, as they become a teenager, with support from you. Read more about asthma in adults.
Asthma and your child (Asthma UK)(external link) Take a look at a range of topics on childhood asthma. These are British resources so may include content that is not relevant to a NZ audience.
Asthma in under five-year-olds(external link) Goodfellow Podcast, NZ, 2020 Dr David McNamara talks through addressing the challenges and barriers to diagnosis of asthma in the under five-year-old child.
Video: Goodfellow Unit MedTalk – paediatric asthma
"Dr Diana North, (Goodfellow Unit GP Advisor) talks with Dr David McNamara, (Paediatric Respiratory and Sleep Medicine Specialist employed at Auckland's Starship Children's Hospital) about what is new in the diagnosis and management of asthma in children up to 16 years of age." This video may take a few moments to load.
(Goodfellow Unit, NZ, 2017)
Course
Asthma and COPD Fundamentals Course(external link) Asthma & Respiratory Foundation NZ This course aligns the latest research with specific information for the New Zealand context, such as recently funded medications, treating Māori and Pasifika peoples, and best practice health literacy. The course aligns with the latest New Zealand asthma guidelines. It includes two half day workshops covering the key aspects of COPD and asthma pathophysiology, management and practice.