Actinic keratoses is skin damage caused by years of exposure to ultraviolet (UV) radiation found in sunlight.
Low or no data? Visit zero.govt.nz, scroll down the page then click on our logo to return to our site and browse for free.
Actinic keratoses | Mate kiri hakihaki
Also known as solar keratoses
Key points about actinic keratoses
- Actinic keratoses (mate kiri hakihaki) are flat, scaly areas that develop on skin damaged by ultraviolet (UV) light from the sun.
- Actinic keratoses are precancerous lesions.
- If left untreated they can sometimes progress to become a type of non-melanoma skin cancer called squamous cell carcinoma.
- Actinic keratoses tend to occur on sun-exposed areas such as your face, ears, scalp, forehead, hands and legs.
- Actinic keratoses are most common in people with fair skin or those who have worked outdoors for long periods without skin protection.

The aim of treatment is to remove the abnormal skin cells to prevent them becoming skin cancers. New skin then forms from deeper cells that have escaped sun damage.
Treatment will depend on the size and extent of the skin lesions and may include the following:
- Cryotherapy – freezing with liquid nitrogen. This is a very common treatment that is easy to do. It may leave a pale scar and often needs repeating.
- Topical creams – a range of creams are available. These are useful for treating areas that are not suitable for other treatments or for large areas where there are multiple keratoses, such as on your scalp, forehead or ears. Examples of topical creams include 5-Fluorouracil cream and Imiquimod.
- Photodynamic therapy (PDT) – this involves applying a photosensitiser (a porphyrin chemical) to the affected area before exposing it to a strong source of visible light. The treated area develops a 'burn' and then heals over a couple of weeks or so. Metvix PDT is available in New Zealand.
- Excision – this involves a small surgical procedure using local anaesthetic to cut the lesion out. This will often need a few sutures (stitches), which are removed 5 to 14 days later (depending on the location).
If actinic keratoses are widespread, it may not be practical to treat all lesions. In that case, your doctor will focus on the most thickened, tender or annoying ones. The thicker and tender ones are at greatest risk of progressing to skin cancer.
The best option for preventing actinic or solar keratoses from developing or getting worse is to protect your skin from the sun and UV rays.
Regularly check all your skin (from head to toe). If you see anything that is growing, bleeding or in any way changing, go and see your doctor straight away.
See skin checks.
Ways to protect your skin
- Avoid outdoor activities when the sun is strongest – between 10am and 4pm from September to April in New Zealand.
- Wear sunscreen and lip balm daily that offer SPF 30 or higher sun protection.
- Use sunscreen that offers broad-spectrum (UVA/UVB) protection and is water resistant.
- Apply the sunscreen and lip balm to dry skin 15 minutes before going outdoors.
- Apply the sunscreen to every part of your body that will not be covered by clothing. Reapply it every 2 hours if you are swimming or sweating.
- Whenever possible, wear a wide-brimmed hat, long sleeves and long pants.
- Wear sunglasses to protect the skin around your eyes.
- Avoid getting a tan and never use a tanning bed or sun lamp.
See also sun safety.
Skin cancers(external link)(external link) BPAC, NZ, 2017
Solar keratoses information sheet(external link)(external link) British Association of Dermatologists, UK, 2020
Actinic keratoses(external link)(external link) NHS, UK, 2014
Resources
Signs of skin cancer(external link) Cancer Society, NZ, 2010
Detecting & diagnosing skin cancer (external link)Cancer Society, NZ, 2014
Skin cancer in New Zealand(external link) SunSmart, NZ, 2018
Finding skin cancer early could save your life (external link)Melanoma NZ and Health Promotion Agency, NZ, 2019
|
The content on this page will be of most use to clinicians, such as nurses, doctors, pharmacists, specialists and other healthcare providers. |
From How to use fluorouracil and imiquimod for non-melanoma skin cancer in a general practice setting(external link)(external link) BPAC, NZ, 2017
Actinic keratoses are benign but can progress to invasive malignant disease if left untreated. Surgical excision is not routinely performed, due to the nature of the lesions. However, some actinic keratoses may be hypertrophic, in which case shave excision can be performed. Biopsy is not usually necessary for an isolated lesion of typical appearance, but should be considered for patients with recurrent lesions or if the diagnosis is unclear.
Treatment summary
- Isolated scaly lesions – cryotherapy or surgical excision if the lesion is resistant to cryotherapy and hyperkeratotic.
- Isolated flat lesions – imiquimod, fluorouracil (or ingenol gel).
- Clustered lesions – cryotherapy initially to scaly lesions, followed by field treatment with imiquimod or fluorouracil (or ingenol gel or photodynamic therapy).
- Atypical lesions with suspected malignancy – surgical excision.
Other resources
Actinic keratoses(external link)(external link) Dermnet, NZ, 2015
See our page Skin cancer for healthcare providers
Brochures

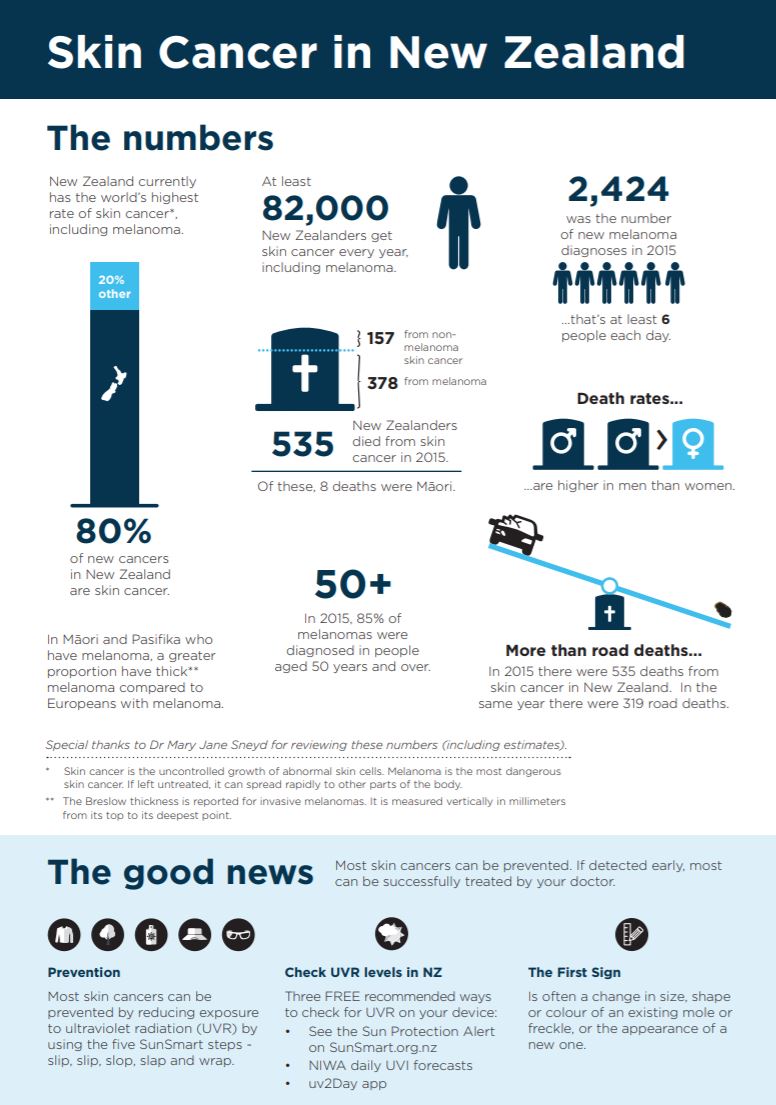
Skin cancer in New Zealand(external link)
SunSmart, NZ, 2018
Signs of skin cancer(external link)
Cancer Society, NZ, 2010
Need help now?



Credits: Healthify editorial team. Healthify is brought to you by Health Navigator Charitable Trust.
Reviewed by: Dr Karen Koch, consultant dermatologist, Auckland
Last reviewed:
Page last updated:
